The Scale of the Problem
Substance use disorders affect approximately 46.3 million Americans aged 12 and older, according to the 2021 National Survey on Drug Use and Health (NSDUH) conducted by SAMHSA. Yet only about 10% of those who need treatment actually receive it. While many factors contribute to this treatment gap—including stigma, lack of awareness, and personal reluctance—one of the most powerful and least discussed barriers is geography.
Where you live in America can dramatically influence whether you have access to evidence-based addiction treatment. From facility density to insurance acceptance rates, the landscape of care varies enormously from state to state, county to county, and even neighborhood to neighborhood. This article examines the data behind these disparities and explores potential solutions.
What Are Treatment Deserts?
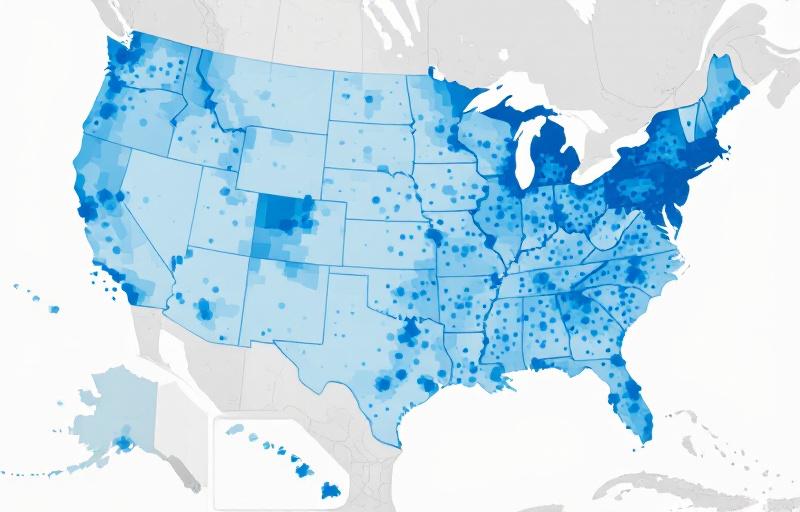
A "treatment desert" is an area where individuals must travel excessive distances—often 25 miles or more in urban areas and 50+ miles in rural regions—to reach the nearest addiction treatment facility. According to data compiled by RehabAnalytics from SAMHSA's National Directory of Drug and Alcohol Abuse Treatment Facilities, approximately 1 in 5 Americans lives in a county with zero or only one specialized treatment provider.
These deserts are not random. They disproportionately affect communities that are already vulnerable: rural areas with aging populations, historically underfunded tribal communities, and economically distressed regions where healthcare infrastructure has been systematically eroded. The National Institute on Drug Abuse (NIDA) has noted that overdose death rates in many rural counties now exceed those in urban areas, even as treatment resources remain concentrated in metropolitan centers.
The consequences are measurable. Research published in the Journal of Substance Abuse Treatment found that individuals living more than 30 minutes from the nearest treatment facility were 40% less likely to initiate treatment and 60% less likely to complete a full course of care. Every additional mile between a patient and a provider represents an exponential drop in the probability of recovery.
Rural vs. Urban Disparities
The rural-urban divide in addiction treatment access is one of the starkest healthcare inequities in America. According to SAMHSA data, metropolitan areas have an average of 31.2 treatment facilities per 100,000 residents, compared to just 11.7 per 100,000 in nonmetropolitan areas. But raw facility counts tell only part of the story.
Rural treatment facilities tend to offer fewer services, accept fewer insurance types, and employ fewer specialized clinicians. A rural facility may provide outpatient counseling but lack the capacity for medically supervised detoxification, medication-assisted treatment (MAT), or dual diagnosis programming. This means that even when a facility exists nearby, it may not offer the level of care a patient needs.
Transportation compounds the problem. In rural areas, public transit is often nonexistent, and many patients lack reliable personal vehicles. Programs that require daily attendance—such as intensive outpatient programs (IOPs) or methadone maintenance—become impractical when they require a 90-minute drive each way.
Cultural factors also play a role. Rural communities often have stronger stigma around substance use disorders, making individuals less likely to seek help even when services are available. Privacy concerns are amplified in small towns where "everyone knows everyone," and patients may fear being seen entering a treatment facility.
Insurance and Financial Barriers
Geographic disparities in treatment access are closely intertwined with insurance coverage gaps. States that expanded Medicaid under the Affordable Care Act (ACA) saw significant increases in treatment admissions—an average of 18% higher than non-expansion states, according to a 2020 analysis in the American Journal of Public Health. Yet 10 states have still not expanded Medicaid, leaving millions of low-income adults without coverage for substance use treatment.
Even in expansion states, the picture is complicated. Many treatment facilities do not accept Medicaid, and those that do often have long waiting lists. SAMHSA's National Survey of Substance Abuse Treatment Services (N-SSATS) reveals that only 62% of treatment facilities nationwide accept Medicaid, and only 73% accept private insurance. The remainder operate on a cash-only or sliding-fee basis, creating additional barriers for patients who cannot pay out of pocket.
The financial burden of treatment varies dramatically by region. In states with robust public funding for substance use services—such as Connecticut, Vermont, and Oregon—patients have access to a wider range of publicly funded programs. In states with minimal public investment, such as Texas and Mississippi, patients often face impossible choices between seeking treatment and meeting basic needs like housing and food.
The Workforce Shortage
Behind every treatment facility gap is a workforce crisis. The addiction treatment field has long struggled with recruitment and retention, and these challenges are especially acute in underserved areas. SAMHSA estimates that the United States needs approximately 28,000 additional addiction counselors and 6,000 additional addiction psychiatrists to meet current demand.
Rural areas face the most severe shortages. Fewer than 7% of psychiatrists and 12% of licensed addiction counselors practice in rural communities, despite these areas representing nearly 20% of the U.S. population. Low salaries, professional isolation, and limited career advancement opportunities make it difficult to attract qualified clinicians to underserved regions.
The workforce problem also affects quality of care. Facilities in underserved areas are more likely to rely on paraprofessional staff with limited training and less likely to offer evidence-based modalities such as cognitive behavioral therapy (CBT) or contingency management. This creates a two-tiered system where the quality of care available depends largely on where a patient happens to live.
Telehealth as a Bridge
The COVID-19 pandemic accelerated the adoption of telehealth for addiction treatment, and this shift has shown remarkable promise in bridging geographic access gaps. During 2020–2021, the DEA's emergency authorization allowing telemedicine prescribing of buprenorphine (a key medication for opioid use disorder) led to a 30% increase in buprenorphine prescriptions in rural counties, according to data from the CDC.
Telehealth removes many of the barriers that make in-person treatment inaccessible: transportation, childcare, work conflicts, and privacy concerns are all reduced when treatment can be accessed from home. Virtual intensive outpatient programs (IOPs), online therapy sessions, and remote medication management have proven effective in clinical trials, with outcomes comparable to in-person care for many populations.
However, telehealth is not a complete solution. Digital infrastructure gaps—including limited broadband access in rural areas—create their own barriers. The FCC estimates that approximately 21 million Americans lack access to reliable high-speed internet, with rural communities disproportionately affected. Additionally, certain treatment modalities, such as residential programs, medically supervised detoxification, and group therapy, lose effectiveness when delivered remotely.
The most promising models combine telehealth with strategic in-person touchpoints. Hub-and-spoke systems, where a central treatment center provides specialized services while satellite locations offer telehealth-enabled primary care, have shown success in states like Vermont and California. These hybrid models can extend the reach of specialized clinicians while maintaining the human connection that many patients need.
State-Level Funding Variations
Public funding for substance use treatment varies enormously across states, creating geographic inequities that compound existing access problems. According to the National Association of State Alcohol and Drug Abuse Directors (NASADAD), per-capita state spending on substance use treatment ranges from less than $10 in some states to over $100 in others.
States with higher per-capita funding tend to have more treatment facilities, shorter wait times, greater service diversity, and better patient outcomes. They are also more likely to fund prevention programs, which reduce the downstream demand for treatment services. Conversely, states that underinvest in treatment infrastructure often see higher rates of emergency department visits, hospitalizations, and overdose deaths—costs that ultimately fall on taxpayers through higher healthcare spending.
Federal funding through SAMHSA's Substance Abuse Prevention and Treatment Block Grant (SABG) provides a baseline level of support, but it represents only a fraction of total treatment spending. The allocation formula for SABG funding does not adequately account for geographic variations in need, meaning that states with the most severe treatment gaps do not necessarily receive proportionally more federal support.
Policy Recommendations
Addressing the geography of addiction treatment access requires coordinated action at the federal, state, and local levels. Based on the evidence reviewed above, RehabAnalytics recommends the following policy priorities:
1. Expand Medicaid in all remaining states. The data is unambiguous: Medicaid expansion increases treatment access and reduces overdose deaths. Federal incentives should be strengthened to encourage the remaining non-expansion states to act.
2. Invest in workforce development. Loan forgiveness programs, rural practice incentives, and expanded training pipelines for addiction counselors and prescribers would help address the critical workforce shortage in underserved areas.
3. Make telehealth flexibilities permanent. The emergency-era telehealth authorizations for substance use treatment should be codified into permanent federal regulations, ensuring that patients can continue accessing care remotely when appropriate.
4. Modernize SABG funding formulas. Federal block grant allocations should be updated to reflect current epidemiological data and geographic need, directing more resources to areas with the greatest treatment gaps.
5. Support hub-and-spoke delivery models. Federal and state grants should incentivize the development of hybrid treatment networks that combine centralized specialty services with distributed, telehealth-enabled access points.
The geography of addiction does not have to be destiny. With targeted investment, innovative delivery models, and policy reform, it is possible to ensure that every American—regardless of zip code—has meaningful access to the treatment they need.
Need Help Finding Treatment?
RehabAnalytics can help you locate verified treatment facilities in your area. Our database covers over 14,000 programs nationwide, with detailed information on services, insurance acceptance, and patient outcomes.
(855) 312-7200Sources
- SAMHSA. (2022). 2021 National Survey on Drug Use and Health.
- NIDA. (2023). Trends & Statistics: Drug Use and Health.
- SAMHSA. (2023). National Survey of Substance Abuse Treatment Services (N-SSATS).
- American Journal of Public Health. (2020). Medicaid Expansion and Substance Use Treatment Admissions.
- Federal Communications Commission. (2021). Broadband Deployment Report.